POLYMORPHISM OF THE ARYLAMINE-N-ACETYLTRANSFERASE GENE
IN ENDOMETRIOSIS PATIENTS IN THE REPUBLIC OF BASHKORTOSTAN
Iskhakova GM1,*, Abazova EF2, Viktorova TV1, Kudakaeva LR1
*Corresponding Author: Dr. Gulnaz M. Iskhakova, Department of ?, Bashkir State Medical University, 450000 Ufa, Lenina St. 3, Russia; Tel.: +007-347-273-5875; Fax: +007-347-272-3751; E-mail: iskhakov_vr@ rambler.ru
page: 55
|
|
RESULTS AND DISCUSSION
Of the endometriosis patients, 48.0% were from 41 to 50 years old, 87.0% suffered from algodysmenorrhea, 82.4% from chronic pelvic pain, 49.0% had problems with their menstrual cycles and 44.0% were infertile. The prevailing nosologic forms were: focal womb endometriosis (32.9%), diffusive womb endometriosis (25.5%) and extensive endometriosis (17.0%). Some 91.5% of the patients suffered from accompanying diseases, with anemia with cardiovascular system diseases and gastrointestinal diseases being present in 24.2 and 27.3%, respectively. A combination of endometriosis and womb myoma was preset in 39.1%, and 23.7% had chronic inflammatory diseases of womb and uterine appendages. The patients were prescribed dufaston or danazol. This treatment could be considered effective, if the pain syndrome had abated, the menstrual cycle had become normal, there had been positive dynamics of the results of ultrasound examination and hysteroscopy. Fifty-four patients received hormonal treatment, of whom 32 (59.3%) gave a positive result.
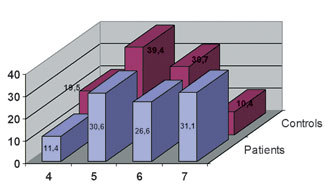
There were more slow acetylators (S) among the endometriosis patients [77.4% as compared with 62.2% in the control group; λ2 = 8.276; p = 0.0210, odds ratio (OR) = 2.08) (Table 2). The distribution of the allele frequencies of the NAT2 gene in endometriosis patients and in controls is presented in Figure 1.
The prevailing allele in the control group was NAT2*5 (39.4%) vs. 30.6% in the endometriosis group (λ2 = 3.8625; p = 0.0494). This NAT2*5 is the most widespread, occurring in 44.0 to 47.0% of the Caucasian population [4]. Nat2*4 without any signs of mutation was present in 11.9% of endometriosis patients and in 19.5% of the controls (λ2 = 5.2189; p = 0.0228; OR = 1.8323). This suggests that, NAT2*4 and NAT2*5 are protective alleles. NAT2*7 was present in 31.1% of endometriosis patients (λ2 = 31.3488, p = 0.0005; OR = 3.8972). In the European population, its frequency is 1.0 to 3.0%, but in the population of the Volgo-Ural region its frequency is 10.2% [4,22]. In our control group, its frequency was 10.4%. We found that NAT2*7 is a marker for endometriosis. The index of OR was 3.9 [confidence interval (CI) = 2.3352-6.5370]. NAT2*6 was found in 26.6% of the endometriosis patients and in 30.7% of the controls. The distribution of the NAT2 gene genotypes in endometriosis patients and in controls is presented in the Table 3.
The number of genotypes in the endometriosis patients was 16 vs. 14 in the controls. There protective genotypes NAT2*4/*5, NAT2*4/*6 and NAT2*5/*6 had a total frequency of 22.6% in the endometriosis group and 53.8% in the controls. Genotypes NAT2*6/*6/*7, NAT2*6/*7/*7, NAT2*7/*7 were found only in endometriosis patients, with a total frequency of 13.7%. Genotypes of high risk such as NAT2*5/*6/*7, NAT2*5/*7/*7, NAT2*6/*6/*7, NAT2*6/*7/*7 and NAT2*7/*7 had a total frequency of 34.3% in the endometriosis group and 5.0% in the controls. There were 43.1% of slow acetylators with more than two mutant alleles in the endometriosis patients, but only 10.9% in the control group (λ2 = 28.1181; p = 0.0005). The index of OR was 6.19.
The very slow acetylators prevailed in the patients with extensive endometriosis, focal womb endometriosis and ovary endometriosis (58.8, 54.5 and 50.0%, respectively) but were less frequent in those with endometriosis of the neck of the womb (30.8%). Slow acetylators were more frequent among those with diffusive womb endometriosis and endometriosis of the neck of the womb (44.0 and 46.1%, respectively). The frequency of R carriers in patients with endometriosis and infertility in anamnesis was twice as high as that among the other patients (11.6 and 5.9%, respectively).
We have studied the effectiveness of hormonal treatment in relation to the NAT2 gene polymorphism in endometriosis patients. There prevailed in individuals with the genotypes that contained more than one mutant allele in the group of patients sensitive to pharmacotherapy (78.8%). In individuals with the NAT2*4/4 gene, the treatment was effective in only 3.0% of cases, and was not effective in 13.6% of cases.
These results indicate that inactivation of xenobiotics, including drugs, occur in endometriosis patients with the NAT2*4/4 genotype, whereas individuals with mutant alleles in the genotype benefit from slower inactivation of drugs and this may stipulate for higher effectiveness of the therapy. They also indicate that unfavorable NAT2 alleles have a role in the pathogenesis of endometriosis and influence the effectiveness of therapy.
Table 2. Distribution of the phenotype frequencies
|
|
n |
Frequency of Phenotypes
According to the NAT2 Gene |
|
|
|
R
Absolute (%) |
S
Absolute (%) |
|
Patients |
102 |
23 (22.6) |
79 (77.4) |
|
Controls |
119 |
45 (37.8) |
74 (62.2) |
|
c2; p |
5.314; 0.022 |
 NAT2/Kpnl NAT2/Kpnl
 NAT2/Tagl NAT2/Tagl
 NAT2/BamHI NAT2/BamHI
Figure 1. Distribution of the NAT2 alleles in endometriosis patients.
Table 3. Polymorphism of the NAT2 gene
|
|
Patients (n = 102) |
Controls (n = 119) |
|
NAT2 Genotype |
Absolute |
% |
Absolute |
% |
|
*4/*4 |
6 |
5.9 |
5 |
4.2 |
|
*4/*5 |
7 |
6.9 |
20 |
16.8 |
|
*4/*6 |
4 |
3.9 |
14 |
11.8 |
|
*4/*7 |
6 |
5.9 |
5 |
4.2 |
|
*5/*5 |
3 |
2.9 |
12 |
10.1 |
|
*5/*5/*6 |
4 |
3.9 |
2 |
1.7 |
|
*5/*5/*7 |
6 |
5.9 |
3 |
2.5 |
|
*5/*6 |
12 |
11.8 |
30 |
25.2 |
|
*5/*6/*6 |
3 |
2.9 |
2 |
1.7 |
|
*5/*6/*7 |
16 |
15.7 |
5 |
4.2 |
|
*5/*7 |
7 |
6.9 |
7 |
5.9 |
|
*5/*7/*7 |
5 |
4.9 |
1 |
0.8 |
|
*6/*6 |
0 |
0.0 |
9 |
7.6 |
|
*6/*6/*7 |
5 |
4.9 |
0 |
0.0 |
|
*6/*7 |
9 |
8.8 |
4 |
3.4 |
|
*6/*7/*7 |
5 |
4.9 |
0 |
0.0 |
|
*7/*7 |
4 |
3.9 |
0 |
0.0 |
|
Alleles |
|
4 |
29 |
11.7 |
49 |
19.5 |
|
5 |
76 |
30.6 |
99 |
39.4 |
|
6 |
66 |
26.6 |
77 |
30.7 |
|
7 |
77 |
31.1 |
26 |
10.4 |
Figure 2. The distribution of the frequencies of NAT2 genotypes in endometriosis patients
|
|
|
|

 |
Number 28
Vol 28 2025 Supplement |
Number 27
VOL. 27 (2), 2024 |
Number 27
VOL. 27 (1), 2024 |
Number 26
Number 26 VOL. 26(2), 2023 All in one |
Number 26
VOL. 26(2), 2023 |
Number 26
VOL. 26, 2023 Supplement |
Number 26
VOL. 26(1), 2023 |
Number 25
VOL. 25(2), 2022 |
Number 25
VOL. 25 (1), 2022 |
Number 24
VOL. 24(2), 2021 |
Number 24
VOL. 24(1), 2021 |
Number 23
VOL. 23(2), 2020 |
Number 22
VOL. 22(2), 2019 |
Number 22
VOL. 22(1), 2019 |
Number 22
VOL. 22, 2019 Supplement |
Number 21
VOL. 21(2), 2018 |
Number 21
VOL. 21 (1), 2018 |
Number 21
VOL. 21, 2018 Supplement |
Number 20
VOL. 20 (2), 2017 |
Number 20
VOL. 20 (1), 2017 |
Number 19
VOL. 19 (2), 2016 |
Number 19
VOL. 19 (1), 2016 |
Number 18
VOL. 18 (2), 2015 |
Number 18
VOL. 18 (1), 2015 |
Number 17
VOL. 17 (2), 2014 |
Number 17
VOL. 17 (1), 2014 |
Number 16
VOL. 16 (2), 2013 |
Number 16
VOL. 16 (1), 2013 |
Number 15
VOL. 15 (2), 2012 |
Number 15
VOL. 15, 2012 Supplement |
Number 15
Vol. 15 (1), 2012 |
Number 14
14 - Vol. 14 (2), 2011 |
Number 14
The 9th Balkan Congress of Medical Genetics |
Number 14
14 - Vol. 14 (1), 2011 |
Number 13
Vol. 13 (2), 2010 |
Number 13
Vol.13 (1), 2010 |
Number 12
Vol.12 (2), 2009 |
Number 12
Vol.12 (1), 2009 |
Number 11
Vol.11 (2),2008 |
Number 11
Vol.11 (1),2008 |
Number 10
Vol.10 (2), 2007 |
Number 10
10 (1),2007 |
Number 9
1&2, 2006 |
Number 9
3&4, 2006 |
Number 8
1&2, 2005 |
Number 8
3&4, 2004 |
Number 7
1&2, 2004 |
Number 6
3&4, 2003 |
Number 6
1&2, 2003 |
Number 5
3&4, 2002 |
Number 5
1&2, 2002 |
Number 4
Vol.3 (4), 2000 |
Number 4
Vol.2 (4), 1999 |
Number 4
Vol.1 (4), 1998 |
Number 4
3&4, 2001 |
Number 4
1&2, 2001 |
Number 3
Vol.3 (3), 2000 |
Number 3
Vol.2 (3), 1999 |
Number 3
Vol.1 (3), 1998 |
Number 2
Vol.3(2), 2000 |
Number 2
Vol.1 (2), 1998 |
Number 2
Vol.2 (2), 1999 |
Number 1
Vol.3 (1), 2000 |
Number 1
Vol.2 (1), 1999 |
Number 1
Vol.1 (1), 1998 |
|
|
|